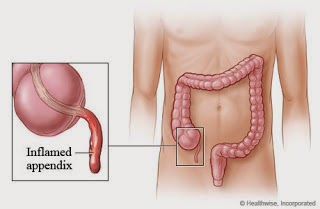
Appendicitis is swelling (inflammation) of the appendix. The appendix is a small pouch attached to the beginning of your large intestine .. that pouch is known as caecum. What causes appendix? Appendicitis occurs when the appendix becomes blocked, often by stool, a foreign body, or cancer. Blockage may also occur from infection, since the appendix swells in response to any infection in the body. The cause of appendicitis isn't always clear. Sometimes appendicitis can occur as a result of: An obstruction. Food waste or a hard piece of stool (fecal stone) can block the opening of the cavity that runs the length of your appendix. An infection. Appendicitis may also follow an infection, such as a gastrointestinal viral infection, or it may result from other types of inflammation. In both cases, bacteria inside the appendix multiply rapidly, causing the appendix to become inflamed, swollen and filled with pus. If not treated promptly, the appendix can rupture. Symptoms of appen...



Comments
Post a Comment