Medical

The first symptom of breast cancer most women notice is a lump or an area of thickened tissue in their breast. Most lumps (90%) are not cancerous, but it is always best to have them checked by your doctor.
See your GP if you notice any of the following:
a lump or area of thickened tissue in either breast
a change in the size or shape of one or both breasts
discharge from either of your nipples (which may be streaked with blood)
a lump or swelling in either of your armpits
dimpling on the skin of your breasts
a rash on or around your nipple
a change in the appearance of your nipple, such as becoming sunken into your breast

SNAKE BITES
Snake bite is a well-known occupational hazard amongst farmers, plantation workers, and other outdoor workers and results in much morbidity and mortality throughout the world. This occupational hazard is no more an issue restricted to a particular part of the world; it has become a global issue. Accurate statistics of the incidence of snakebite and its morbidity and mortality throughout the world does not exist; however, it is certain to be higher than what is reported. This is because even today most of the victims initially approach traditional healers for treatment and many are not even registered in the hospital. Hence, registering such patients is an important goal if we are to have accurate statistics and reduce the morbidity and mortality due to snakebite. World Health Organization/South East Asian Region Organisation (WHO/SEARO) has published guidelines, specific for the South East Asian region, for the clinical management of snakebites. The same guidelines may be applied for managing snakebite patients in other parts of the world also, since no other professional body has come up with any other evidence-based guidelines. In this article we highlight the incidence and clinical features of different types of snakebite and the management guidelines as per the WHO/SEARO recommendation.
Keywords: Anti snake venom, global issue, snakebite
Venomous animals account for much morbidity and mortality. Worldwide, it is estimated that more than 5 million persons per year are bitten by snakes, out of which approximately 100,000 develop severe sequelae.[1,2] The actual figure may be much more since in India alone the mortality is suggested to be around 30,000.[3] Out of the available yearly statistics, the United States alone had 50,000 cases of bites, of which 7000 were by venomous snakes. Interestingly, of those 7,000 snakebite victims, 1,200 did not seek medical attention and yet they fully recovered. In all, there were 15 fatalities and thus the chance of survival is 499 out of 500. According to an epidemiological survey among 19,000 individuals living in 26 villages in Burdwan district (West Bengal), there was an annual incidence of snakebite of 0.16% and a mortality rate of 0.016% per year.[4] Maharashtra reports an incidence of 70 bites per 100,000 population and a mortality of 2.4 per 100,000 persons per year.[5] Indian states with high incidence of snakebites cases are Tamil Nadu, West Bengal, Maharashtra, Uttar Pradesh, and Kerala.[6] In Myanmar (Burma) Russell's vipers are responsible for 90% of cases. In 1991, there were 14,000 bites with 1,000 deaths and in 1997, 8,000 bites with 500 deaths. Under-reporting is estimated at 12%.[7] In Bangladesh, a survey of 10% of the country in 1988–1989 revealed 764 bites with 168 deaths over the 1-year period. Cobra bites (34% of all bites) had a case fatality of 40%. In Vietnam there are an estimated 30,000 bites per year. Among 430 rubber plantation workers bitten by Malayan pit vipers between 1993 and 1998, the case fatality was 22%, but only a minority had received antivenom treatment. Fishermen are still occasionally bitten by sea snakes but rarely reach hospitals alive. Pakistan has an estimated 20,000 snakebite deaths each year.
In Nepal there is an estimated 20,000 snakebites each year, with about 200 deaths in hospitals, mainly in the Terai region. One survey suggested as many as 1,000 deaths per year. Among 16 fatalities recorded at one rural clinic during a monsoon season, 15 had died on their way to seek medical care.[8]
EPIDEMIOLOGY
Agent
Snakes are distributed throughout most of the earth's surface with some exceptions such as the Arctic, Antarctic, and many small islands. Snakes are poikilothermic carnivorous reptiles that have evolved the venomous apparatus for the purpose of procurement of food.[9] To a large extent the manifestation of snakebite depends upon the species of snake, and therefore identification of the type of snake is important. At times the bite mark might not be visible (e.g., in the case of krait). The killed snake brought as evidence helps in identification of snake, in which case species-specific monovalent Anti snake venom (ASV) can be administered. The clinical manifestations of the patient may not correlate with the species of snake brought as evidence. It is therefore advantageous to know the appearance of the snake so as to recognize the species.
The three major families of venomous snakes are the Elapidae, the Viperidae, and the Hydrophidae.
Elapidae (cobra, king cobra, krait, and coral snake): These snakes have heads that are of about the same width as their necks. The head is covered with large scales but lack laureal shields. Their pupils are round and they are oviparous. These snakes have grooved fangs that are short, fixed, and covered by mucous membrane. They, therefore, cannot bite through clothes and usually deliver only a sublethal dose.
Viperidae (vipers): The head of a viper is triangular, wider than the neck, and has laureal shields. They have vertically elliptical pupils and are ovi-viviparous. Their fangs are long, movable, and canalized like hypodermic needles. They are further subdivided into pit viper and pitless viper subfamilies. The Crotalinae (pit vipers) have a special sense organ, the pit organ, to detect their warm-blooded prey. This is situated between the nostril and the eye. The rattlesnake belongs to the pit viper subfamily, while the Russell's viper and the saw-scaled viper belong to the pitless viper subfamily.
Hydrophidae (sea snake): Sea snakes are found in the vicinity of the seacoast. They have a small head and a flattened tail that helps them swim. Though venomous, they seldom bite.
In India, more than 200 species of snakes have been identified but only 52 are poisonous; the common krait (Bungarus caeruleus), Indian cobra (Naja naja), Russell's viper (Daboia russelii), and saw-scaled viper (Echis carinatus) are the most poisonous (“the big four”).[10,11] In the Indian setting, almost two-thirds of bites are attributed to saw-scaled vipers, about one-fourth to Russell's viper, and only a small proportion to cobras and kraits.[12,13]
Host and environmental factors
Thorough statistical analysis of snakebite is difficult and the available data is not always complete because of the varied distribution (and because most bites occur in remote villages). Snakebite may be termed an occupational disease, as farmers, plantation workers, herdsmen, hunters, or workers on development sites are mostly affected.[14] Snakebites show a classical seasonal variation, being more common in summers and in the rainy season, when it is associated with agricultural activities.[3] The majority of snakes do not bite without provocation; most bites are inflicted when the snakes are inadvertently trodden upon. Males are bitten almost twice as often as females,[15] with the majority of the bites being on the lower extremities.[16–18] Fortunately, 50% of bites by venomous snakes are “dry bites” that result in negligible envenomation. The percentage of dry bites ranges from 10–80% for various poisonous snakes.[19]
SNAKE VENOM
Chemical composition
The normal function of snake venom is to immobilize the prey and to assist in digestion. The toxic component of snake venom can be classified into four broad categories: enzymes, polypeptides, glycoproteins, and compounds of low molecular weight.[9] They can also be classified as protein (90–95%) and nonprotein (5–10%) compounds.[9] Table 1 provides the chemical composition of snake venom.
Compounds present in snake venom
Toxic effects of snake venom
The toxic effect of snake venom results from both the protein and the nonprotein component. It is further complicated by the inflammatory response of the victim's body.
Phospholipase A2 is present in the venom of all families of poisonous snakes and is the enzyme that has been most widely studied. Phospholipase A2 inhibits electron transfer at cytochrome C level and renders mitochondrial-bound enzymes soluble. It damages red blood cells, leukocytes, platelets, skeletal muscle, vascular endothelium, peripheral nerve endings, and the myoneural junction.[9]
Hyaluronidase helps spread of venom through tissues, and proteolytic enzymes are responsible for the local edema, blistering, and necrosis.[3]
α- Neurotoxins bind to acetylcholine receptors at the motor end-plate, whereas β- neurotoxins first cause release of acetylcholine at the nerve endings at the myoneural junction and then damage the endings, preventing further release of transmitter.[3] All this leads to a flaccid paralysis of the victim.
Polypeptides, being smaller molecules, are rapidly absorbed into the systemic circulation and cause systemic toxicity in vessel-rich organs (e.g., heart, lung, kidneys, etc.) as well as at pre- and postsynaptic membranes.
CLINICAL FEATURES OF SNAKEBITE
Some people who are bitten by snakes (or suspect or imagine that they have been bitten) may develop quite striking symptoms and signs, even when no venom has been injected. This results from an understandable fear of the consequences of a real venomous bite. Anxious people may hyperventilate so that they develop pins-and-needles sensation in the extremities, spasm of their hands and feet, and dizziness. Others may develop vasovagal shock after the bite or suspected bite, with faintness and collapse with profound slowing of the heart. Others may become highly agitated and irrational and may manifest a wide range of misleading symptoms.[14]
The clinical presentation of a snakebite victim varies with the age and size of the patient, the species of snake, the number and location of the bites, and the quantity and toxicity of the venom.
Morbidity and mortality depends on the age and size of victim (children receive larger envenomation relative to body size) as well as comorbid conditions (elderly patients succumb more easily to snake venom).[9] Other factors affecting severity and outcome are listed in Table 2. Factors not contributing to outcome are size of the snake and time of bite (day/night).[14]
Factors contributing to severity and outcome in snakebite
Elapid bites
Bites by krait, coral snake, and some cobras are associated with minimal local changes; however, bite by the Indian cobra (Naja naja) results in tender local swelling, blistering, and necrosis. Local necrosis causes a picture of “wet gangrene” with a characteristic putrid smell due to the direct cytolytic action of the venom. “Skip lesions” are typical findings. Systemic absorption occurs through venous channels and result in neurotoxic symptoms. Nausea, vomiting, malaise, prostration, and abdominal pain are the usual initial systemic symptoms. Paralysis is heralded by ptosis, followed by ophthalmoplegia. Paralysis of facial, palatal, tongue, and neck muscles follow. Respiratory failure, precipitated by upper airway obstruction and paralysis of intercostals and diaphragm, is the usual cause of death.[3,9]
Viper bites
Viper bite is primarily vasculotoxic. It causes rapidly developing swelling of the bitten part. Local necrosis is mainly ischemic as thrombosis blocks the local blood vessels and causes a dry gangrene. Systemic absorption is slow; it occurs via the lymphatics and leads to lymphangitis. Hemostatic abnormalities are characteristic of viper bites and are the cause of the complications that lead to death. A persistent ooze from the bite mark and the site of the IV cannula is an indication of the altered clotting mechanism. Hemorrhage and increased capillary permeability leads to shock and pulmonary edema. Oliguria ensues, followed by loin pain due to renal ischemia. Renal failure is the common event before death.[3,9]
Sea snake bite
The effects of a sea snake bite are both myotoxic and neurotoxic and result in clinical and pathological changes typical of segmental myopathic lesions in the skeletal muscles. Muscle pains may last for several months unless treated. Myoglobin and potassium released from damaged skeletal muscle can cause renal failure, while the hyperkalemia thus produced may lead to cardiac arrest.[3]
MANAGEMENT OF SNAKEBITE
WHO/SEARO has published guidelines, specific for the South East Asia region, for the clinical management of snakebites; these guidelines appeared in the supplementary issue of the South East Asian Journal of Tropical Medicine and Public Health.[14]
WHO/SEARO guidelines are universally followed. The following management is as per the WHO guidelines
First aid
The aim of first aid is to retard the systemic absorption of venom and prevent life-threatening complications by prompt transport to a medical facility. First aid can be performed by victim himself/herself or by any person who happens to be nearby. Traditionally, first aid included making local incisions or “tattooing” at the site of the bite, attempts at suctioning venom out of the wound, use of tight bands (tourniquets) around the limb, and/or local application of ice packs. None of the traditional remedies have any proven medical benefit. They should be discouraged as they do more harm than good and delay transport to a medical facility. Incision, suction, electric shocks, cryotherapy, or washing the wound are contraindicated as any interference with the wound introduces infection, increases bleeding from the site, and hastens absorption of the venom.
The current guidelines for first aid include the following:
Reassure the victim (70% of all snakebites are by nonvenomous snakes and 50% of bites by venomous species are dry bites[19])
Immobilize the affected limb (by bandage or clothes to hold splint, but tight arterial compression is not recommended)
Promptly transfer of victim to hospital
Pressure immobilization method (PIM) was developed by the Australian Venom Research Unit, University of Melbourne, Australia, for rapidly acting neurotoxic elapid snake venom. As per the PIM, immobilization and bandaging of the bitten part is similar to that done in the case of a sprained ankle. Studies have shown that it is seldom applied correctly[20] in simulated environments and, moreover, mobilizing the limb for more than 10 min nullifies the benefits of even the correctly applied bandage.[21]
In most instances, health care providers, general public, or community health workers are the first responders to come to the aid of the snakebite victim. If outcomes are to be improved, it is vital that they should all be made aware of the importance of immediate immobilization of the limb and transfer to the hospital at the earliest.
Hospital treatment
Emergency care department
When the patient reaches the emergency department, evaluation should begin with the assessment of the airway, breathing, circulatory status, and consciousness.
Urgent resuscitation will be needed in those in shock (cardiovascular toxicity), those with respiratory failure (neurotoxin), and in those who have had cardiac arrest (due to hypoxia, cardiac toxicity, or hyperkalemia from rhabdomyolysis).
Oxygen should be administered to every envenomed patient and a large-bore intravenous catheter should be inserted. A bolus of normal saline or Ringer's lactate should be given to all patients with suspected envenomation. The patient may then be administered specific treatment after a precise history has been taken and thorough physical examination done.
History
Attempts should be made to determine whether a venomous snake has actually bitten the patient and, if so, the severity of the bite [Table 4]. It is essential to establish that the victim has been bitten by a snake and not by some other animal; this can be cross-checked by looking for fang marks and signs of local envenomation. If the victim has brought the snake, identification of the species should be carried out carefully, since crotalids can envenomate even when dead. This is why bringing the killed snake into the ED should be discouraged. Questions should be asked to determine the time elapsed since the snakebite and a brief medical history should be obtained (e.g., date of last tetanus immunization, use of any medication, presence of any systemic disease, and history of allergy).[9]
Assessment of severity of envenomation
Physical examination
During the initial evaluation, the bite site should be examined for signs of local envenomation (edema, petechiae, bullae, oozing from the wound, etc) and for the extent of swelling. The bite site and at least two other, more proximal, locations should be marked and the circumference of the bitten limb should be measured every 15 min thereafter, until the swelling is no longer progressing. The extremity should be placed in a well-padded splint for at least 24 h. Serial measurement of circumference helps in estimating spread of venom and effect of antivenom.[9] Lymph nodes draining the limb should be palpated and the presence of lymphangitic lines noted.
Distal pulses should be checked and monitored if there is presence of gross swelling. The presence of a pulse does not rule out compartment syndrome however, and compartment pressure should be measured directly if there is concern that a compartment syndrome is developing. The diagnosis is established if the compartment pressure, measured directly by inserting a 22G IV cannula and connecting it with manometer, is raised above 55 cm water/saline. Direct measurement is necessary before resorting to fasciotomy since compartment syndrome is rare in snakebite victims and fasciotomy done without correction of hemostatic abnormality may cause the patient to bleed to death.[14]
Clues for severe snake envenomation should be sought.[14] They consist of the following:
Snake identified is a very venomous one
Rapid early extension of local swelling from the site of the bite
Early tender enlargement of local lymph nodes, indicating spread of venom in the lymphatic system
Early systemic symptoms
Early spontaneous systemic bleeding (especially bleeding from the gums)
Passage of dark brown urine
Go to:
LABORATORY INVESTIGATIONS
Although lab tests are of little value in the diagnosis of snake envenomation, they are useful for prognosticating and for making decisions about specific interventions.[22]
Specific investigations
(a) The 20-min whole blood clotting test (20 WBCT): The 20 WBCT is a simple bedside test of coagulopathy to diagnose viper envenomation and rule out elapid bite. It requires a new clean, dry test tube made up of simple glass that has not been washed with any detergent. A few milliliters of fresh venous blood is drawn and left undisturbed in the test tube for 20 min; the tube is then tilted gently. If the blood is still liquid after 20 min, it is evidence of coagulopathy and confirms that the patient has been bitten by a viper. Cobras or kraits do not cause antihemostatic symptoms.[23]
(b) Enzyme linked immunosorbent assay (ELISA): ELISA tests are now available to identify the species involved, based on antigens in the venom.[24] These tests, however, are expensive and not freely available and thus have limited value in diagnosis; at present, they find use mainly in epidemiological studies.
Other nonspecific tests include
Hemogram: The hemogram may show transient elevation of hemoglobin level due to hemoconcentration (because of the increased capillary leak) or may show anemia (due to hemolysis, especially in viper bites). Presence of neutrophilic leucocytosis signifies systemic absorption of venom.[14] Thrombocytopenia may be a feature of viper envenomation.
Serum creatinine: This is necessary to rule out renal failure after viper and sea snake bite.
Serum amylase and creatinine phosphokinase (CPK): Elevated levels of these markers suggests muscle damage (caution for renal damage).
Prothrombin time (PT) and activated partial thromboplastin time (aPTT): Prolongation may be present in viper bite.
Fibrinogen and fibrin degradation products (FDPs): Low fibrinogen with elevated FDP is present when venom interferes with the clotting mechanism.
Arterial blood gas and electrolyte determinations: These test are necessary for patients with systemic symptoms.
Urine examination: Can reveal hematuria, proteinuria, hemoglobinuria, or myoglobinuria. (Arterial blood gases and urine examination should be repeated at frequent intervals during the acute phase to assess progressive systemic toxicity).
Electrocardiogram (ECG): Nonspecific ECG changes such as bradycardia and atrioventricular block with ST-T changes may be seen.[25]
Electroencephalogram (EEG): Recently, EEG changes have been noted in up to 96% of patients bitten by snakes. These changes start within hours of the bite but are not associated with any features of encephalopathy. Sixty-two percent showed grade I changes, 31% cases manifested grade II changes (moderate to severe abnormality), and the remaining 4% showed severe abnormality (grade III). These abnormal EEG patterns were seen mainly in the temporal lobes.[26]
The first blood drawn from the patient should be typed and cross-matched, as the effects of both venom and antivenom can interfere with later cross-matching.
SPECIFIC THERAPY
Anti–snake venom
Anti–snake venom (ASV) are immunoglobulins prepared by immunizing horses with the venom of poisonous snakes and subsequently extracting and purifying the horses' serum. They are the only effective antidote for snake venom. Antivenoms may be species specific (monovalent/monospecific) or may be effective against several species (polyvalent/polyspecific). Antibodies raised against the venom of one species may have cross-neutralizing activity against other venoms, usually that from closely related species. This is known as paraspecific activity. As per the recommendations of WHO, the most effective treatment for snakebite is the administration of monospecific ASV[27]; however, this therapy is not always available to snakebite victims because of its high cost, frequent lack of availability, and the difficulty in correctly identifying the snake.[3]
WHO recommends that if an adequate cold chain is in place, antivenoms should be prepared in the liquid form, since this reduces production costs and avoids the potential adverse physicochemical alterations to the product sometimes brought about by lyophilization. On the other hand, if the integrity of the cold chain cannot be guaranteed, antivenoms should be lyophilized to maintain stability.[19]
Several antivenom preparations are available internationally. In India, polyvalent antivenom prepared by Central Research Institute, Kasauli (HP) is effective against the most common Indian species [Table 5]. Antivenom produced at the Haffkine Corporation, Parel (Mumbai) is effective against the venom of even more species. Table 6 lists ASV producers in India, both in the public as well as the private sector.
Polyvalent anti–snake venom serum produced by Central Research Institute, Kasauli (Himachal Pradesh)
Anti-snake venom producers in India
ASV is supplied in dry powder form and has to be reconstituted by diluting in 10 ml of normal saline/D5 W. Mixing is done by swirling and not by vigorous shaking.
Indications for ASV
The correct use of antivenom is essential and requires an informed evaluation of the patient. Not every poisonous snakebite merits its use. Antivenom treatment carries a risk of severe adverse reactions and in most countries it is costly and may be in limited supply. It should therefore be used only in patients in whom the benefits of antivenom treatment are considered to exceed the risks. Crotalidae polyvalent immune Fab (ovine) (CroFab; FabAV) has recently been approved for use in the United States. CroFab is a venom-specific Fab fragment of immunoglobulin G (IgG) that works by binding and neutralizing venom toxins, facilitating their redistribution away from target tissues and their elimination from the body. It has been demonstrated that these fragments are safe and effective, with a low incidence of sequelae; however, allergic reactions can occur when any animal protein derivatives are administered to human subjects. The overall incidence of immediate and delayed allergic reactions to this product appears so far to be lower than that reported with conventional whole-IgG antivenom.[28] Antivenom is indicated whenever there are signs of systemic envenomation or presence of severe local swelling. See Table 7 for details.
Indications for anti-snake venom
Antivenom therapy
Antivenom should be ideally administered within 4 h of the bite, but is effective even if given within 24 h. The dosage required varies with the degree of envenomation.
Dose of ASV
Despite widespread use of antivenom, there have been virtually no clinical trials to determine the ideal dose.[29] The dosage has remained a matter of much debate. The conventional dosing in our setup is based on the degree of envenomation [Table 8].
Conventional dose of anti-snake venom
WHO/SEARO recommends the dose of antivenom to be the amount required to neutralize the average venom yield when captive snakes are milked of their venom.[27] Published research has indicated that the Russell's viper injects, on average, 63 mg (SD: ± 7 mg) of venom in the first bite.[30,31] As each vial of polyvalent ASV neutralizes 6 mg of Russell's viper venom, the initial dose should be 8–10 vials to ensure that the majority of the victims are covered by the initial dose; this will also help keep the cost of ASV down to acceptable levels.[32] As snakes inject the same amount of venom into children and adults, children should receive the same dose of antivenom as adults.[21]
Response to infusion of antivenom is marked by normalization of blood pressure.[33] Within 15–30 min bleeding stops, though coagulation disturbances may take up to 6 h to normalize. Neurotoxicity begins to improve within the first 30 min, but patients may require 24–48 h for full recovery.[34]
A repeat dose of ASV should be given when there is persistence of blood incoagulability even after 6 h or continued bleeding after 1–2 h of the initial dose. ASV should also be repeated when there are worsening neurotoxic or cardiovascular signs even after 1–2 h.[14]
ASV administration
ASV can be administered either by slow intravenous injection at a rate of 2 ml/min or by intravenous infusion (antivenom diluted in 5–10 ml per kilogram body weight of normal saline or D5 W and infused over 1 h). Slow intravenous injection has the advantage that a doctor or nurse is present during the injection period when there is a risk of some early reaction to the ASV. All patients should be strictly observed for an hour for development of any anaphylactic reaction. Epinephrine should always be kept ready before administration of antivenom.
ASV should never be given locally at the site of the snakebite since it has not been shown to be effective and, moreover, this route of administration is associated with significant risks. For example, it is extremely painful and may increase intracompartmental pressure. Intramuscular injections are also not preferred since ASV is composed of large molecules (IgG or fragments) which are absorbed slowly via lymphatics, making the bioavailability by this route poor as compared to intravenous administration. Other disadvantages include pain on injection and risk of hematoma formation and sciatic nerve damage in patients with hemostatic abnormalities.[14] Intramuscular injections should only be given in settings where intravenous access cannot be obtained and/or the victim cannot be transported to a hospital immediately.
ASV sensitivity testing
ASV sensitivity testing is no longer recommended as a lack of response does not predict the large majority of early (anaphylactic) or late (serum sickness type) reactions.[14] Such testing could also presensitize the patient to the serum protein and, in addition, often delays treatment.
ASV reaction
Approximately 20% patients treated with ASV develop either early or late reaction.[14]
Early anaphylactic reactions occurs within 10–180 min of start of therapy and is characterized by itching, urticaria, dry cough, nausea and vomiting, abdominal colic, diarrhea, tachycardia, and fever. Some patients may develop severe life-threatening anaphylaxis characterized by hypotension, bronchospasm, and angioedema.
Pyrogenic reactions usually develop 1–2 h after treatment. Symptoms include chills and rigors, fever, and hypotension. These reactions are caused by contamination of the ASV with pyrogens during the manufacturing process.
Late (serum sickness–type) reactions develop 1–12 (mean 7) days after treatment. Clinical features include fever, nausea, vomiting, diarrhea, itching, recurrent urticaria, arthralgia, myalgia, lymphadenopathy, immune complex nephritis and, rarely, encephalopathy.
Treatment of ASV reaction
When the patient shows signs of a reaction, antivenom administration must be temporarily stopped and adrenaline (1 in 1000) given intramuscularly in an initial dose of 0.5 mg in adults or 0.01 mg/kg body weight in children. The dose can be repeated every 5–10 min if necessary.
After adrenaline, an anti-H1 antihistamine such as chlorpheniramine maleate (adult dose 10 mg, children 0.2 mg/kg) should be given intravenously. It may be followed by intravenous hydrocortisone (adult dose 100 mg, children 2 mg/kg).
Late (serum sickness–type) reactions usually respond to a 5-day course of oral antihistamine (e.g., chlorpheniramine 2 mg six hourly in adults and 0.25 mg/kg/day in divided doses in children). Patients who fail to respond within 24–48 h should be given a 5-day course of prednisolone (5 mg six hourly in adults and 0.7 mg/kg/day in divided doses in children).
SUPPORTIVE THERAPY
The patient should be moved to an appropriate area of the hospital. The ICU will be required for patients with signs of severe envenomation (coma, respiratory paralysis, hypotension, pulmonary edema, and history of syncope). Patients with presence of fang marks, moderate pain, minimal local edema, erythema, ecchymosis, and no systemic reactions can be treated in the ward under close monitoring. Supportive therapy is required to buy time while the damaged organs recover. The types of supportive care that may be needed is summarized below.
Coagulopathy with bleeding
Coagulopathy usually reverses after ASV treatment. In exceptional cases, when there is severe bleeding or when urgent surgery is necessary, restoration of coagulability can be accelerated by giving fresh frozen plasma, cryoprecipitate (fibrinogen, factor VIII), fresh whole blood, or platelet concentrates.[27]
Neurotoxic symptoms
Antivenom treatment alone cannot be relied upon to save the life of a patient with bulbar and respiratory paralysis. Once there is loss of the gag reflex, failure to cough, or respiratory distress, endotracheal intubation and initiation of mechanical ventilation is indicated. Tracheostomy and placement of a cuffed tracheostomy tube can be done whenever expertise for endotracheal intubation is not available. Since Elapid toxin result in pathophysiological changes resembling those of myasthenia gravis, anticholinesterase drugs can have a useful effect in patients with neurotoxic envenomation, especially in those bitten by cobras. A trial of anticholinesterase should be performed in every patient with neurotoxic envenomation. Injection neostigmine can be given as 50–100 μg/kg 4 hourly or as a continuous infusion. Glycopyrrolate 0.2 mg can be given before neostigmine as, unlike atropine, glycopyrrolate does not cross the blood–brain barrier. Seneviratne and Dissanayake,[15] in a prospective study on the neurological manifestations, disease course, and outcome in neurotoxic envenomation, demonstrated that neostigmine improved the muscle weakness. However, the number of cases in the study was too small for them to make an unequivocal recommendation. They were of the opinion that it would perhaps be reasonable to offer anticholinesterase therapy to those who demonstrate a positive response to the tensilon test or a decremental response to repetitive nerve stimulation.[15]
Care of bitten part
The appearance of an immobile, tensely-swollen, cold, and apparently pulseless snake-bitten limb may suggest to surgeons the possibility of increased intracompartmental pressure, especially if the digital pulp spaces or the anterior tibial compartment are involved. Swelling of envenomed muscle within such tight fascial compartments could result in an increase in tissue pressure above the venous pressure and result in ischemia. However, the classical signs of an intracompartmental pressure syndrome may be difficult to assess in snakebite victims. Fasciotomy should not be contemplated until hemostatic abnormalities have been corrected, otherwise the patient may bleed to death. It has also been reported that fasciotomy worsens the amount of myonecrosis in crotalid snake venom–injected tissue.[35]
As most snakes harbor aerobic as well as anaerobic bacteria in their mouths, a prophylactic course of penicillin (or erythromycin for penicillin-hypersensitive patients) and a single dose of broad spectrum antibiotic course which will cover anaerobes together with a booster dose of tetanus toxoid is recommended.[27]
CONCLUSION
Snakes do not generally attack human beings unless provoked. However, once bitten, a wide spectrum of clinical manifestations may result. The emphasis should be on early and adequate medical management. Delayed medical management and lack of public awareness results in prolonged hospital and ICU stay of the patients. This can be decreased if regular public programmes regarding prevention, prehospital management (first aid), and the importance of early transfer to hospital are conducted.
Overemphasis on reducing the load of snake venom in the victim during prehospital management can be dangerous because its role is debatable and too much valuable time is wasted in its administration. Most of the traditional methods for first aid treatment of snakebite, both western and “traditional/herbal,” have been found to result in more harm than good. Identification of the species of snake responsible for the bite is important for optimal clinical management. Antivenom is the only effective antidote for snake venom. However, it is expensive and usually in short supply and its use carries the risk of potentially dangerous reactions.

Meningitis is an inflammation of the membranes (meninges) surrounding your brain and spinal cord.
The swelling associated with meningitis often triggers the "hallmark" signs and symptoms of this condition, including headache, fever and a stiff neck.
Most cases of meningitis in the U.S. are caused by a viral infection, but bacterial and fungal infections also can lead to meningitis. Depending on the cause of the infection, meningitis can get better on its own in a couple of weeks — or it can be a life-threatening emergency requiring urgent antibiotic treatment.
If you suspect that you or someone in your family has meningitis, seek medical care right away. Early treatment of bacterial meningitis can prevent serious complications.
Meningitis
Meningitis can be difficult to diagnose.It usually comes on suddenly and can be confused with flu because many of the symptoms are the same.Seek immediate medical help if you notice any of the signs and symptoms of meningitis, particularly in a young child.This may mean going to your local accident and emergency (A&E) department in the middle of the night. Don't wait for the purple rash to appear, because not everyone gets a rash.
Symptoms
Fever and/or vomiting Severe headache Limb, joint, muscle pain Limb/joint/muscle pain (sometimes with pain/diarrhoea)Cold hands and feet, shivering Pale or mottled skin Breathing fast, breathlessness Rash Rash (anywhere on the body) Stiff neck Stiff neck (less common in young children)Dislike of bright lights (less common in young children)Very sleepy Confused, delirious Seizures may also be seen -
Confirming the diagnosis
If meningitis is suspected, treatment will usually begin before the diagnosis has been confirmed. This is because some of the tests can take several hours to complete, and it could be dangerous to delay treatment.The doctors will carry out a physical examination to look for signs of meningitis or septicaemia (blood poisoning), such as a rash. They will also carry out tests to confirm the diagnosis.Diagnostic tests for meningitis may include:a blood test – to check for the presence of bacteria or viruses that can cause meningitisa lumbar puncture – where a sample of cerebrospinal fluid (CSF) is taken from the base of the spine under local anaesthetic and checked for the presence of bacteria or virusesa computerised tomography (CT) scan – if there are any other suspected problems, such as brain damagea chest X-ray – to look for signs of infection

Bacterial Vaginosis
Chlamydia
Genital Herpes
Gonorrhea
Hepatitis B
Hepatitis C
Human Papillomavirus
Lymphogranuloma Venereum (LGV)
Pubic Lice (Crabs)
Scabies
Syphilis
Trichomoniasis
Chancroid
Pelvic Inflammatory Disease (PID)
Scabies

Obesity is a term used to describe somebody who is very overweight, with a lot of body fat.
It's a common problem, estimated to affect around one in every four adults and around one in every five children aged 10 to 11 in the UK.
Defining obesity
There are many ways in which a person's health in relation to their weight can be classified, but the most widely used method is body mass index (BMI).
BMI is a measure of whether you're a healthy weight for your height. You can use the BMI healthy weight calculatorto work out your score.
For most adults:
- a BMI of 25 to 29.9 means you are considered overweight
- a BMI of 30 to 39.9 means you are considered obese
- a BMI of 40 or above means you are considered severely obese
BMI is not used to definitively diagnose obesity – as people who are very muscular sometimes have a high BMI, without excess fat – but for most people, it can be a useful indication of whether they may be overweight.
A better measure of excess fat is waist circumference, and can be used as an additional measure in people who are overweight (with a BMI of 25 to 29.9) or moderately obese (with a BMI of 30 to 34.9).
Generally, men with a waist circumference of 94cm or more and women with a waist circumference of 80cm or more are more likely to develop obesity-related health problems.
Human immunodeficiency virus infection / acquired immunodeficiency syndrome (HIV/AIDS) is a disease of the human immune system caused by infection with human immunodeficiency virus (HIV). The term HIV/AIDS represents the entire range of disease caused by the human immunodeficiency virus from early infection to late stage symptoms. During the initial infection, a person may experience a brief period of influenza-like illness. This is typically followed by a prolonged period without symptoms. As the illness progresses, it interferes more and more with the immune system, making the person much more likely to get infections, including opportunistic infections and tumorsthat do not usually affect people who have working immune systems.

CAUSES
HIV is not spread to a person who donates blood or organs. People who
donate organs are never in direct contact with people who receive them.
Likewise, a person who donates blood is never in contact with the person
receiving it. In all these procedures, sterile needles and instruments
are used.
But HIV can be spread to a person receiving blood or organs from an
infected donor. To reduce this risk, blood banks and organ donor
programs check (screen) donors, blood, and tissues thoroughly.
People at high risk of getting HIV include:
Injection drug users who share needles
Infants born to mothers with HIV who did not receive HIV treatment
during pregnancy
People who have unprotected sex, especially with people who have other
high-risk behaviors, are HIV-positive, or have AIDS
People who received blood transfusions or clotting products between 1977
and 1985, before screening for the virus became standard practice
Sexual partners of those who engage in high-risk activities (such as
injection drug use or anal sex)
After HIV infects the body, the virus has been found in saliva, tears,
nervous system tissue and spinal fluid, blood, semen (including pre-
seminal fluid, which is the liquid that comes out before ejaculation),
vaginal fluid, and breast milk. Only blood, semen, vaginal secretions,
and breast milk have been shown to transmit infection to others.
SYMPTOMS
Symptoms related to acute HIV infection (when a person is first
infected) are often flu-like:
Diarrhea
Fever
Headache
Mouth sores, including yeast infection (thrush)
Muscle stiffness or aching
Night sweats
Rashes of different types
Sore throat
Swollen lymph glands
Many people have no symptoms when they are diagnosed with HIV.
Common symptoms are:
Chills
Fever
Rash
Sweats (particularly at night)
Swollen lymph glands
Weakness
Weight loss
PREVENTION
Preventing HIV/AIDS:
Do not use illegal drugs and do not share needles or syringes. Many
communities now have needle exchange programs, where you can get rid of
used syringes and get new, sterile ones. These programs can also refer
you for addiction treatment.
Avoid contact with another person's blood. If possible, wear protective
clothing, masks, and goggles when caring for people who are injured.
If you test positive for HIV, you can pass the virus to others. You
should not donate blood, plasma, body organs, or sperm.
HIV-positive women who plan to get pregnant should talk to their health
care provider about the risk to their unborn child. They should also
discuss methods to prevent their baby from becoming infected, such as
taking medicines during pregnancy.
Breastfeeding should be avoided to prevent passing on HIV to infants
through breast milk.
Safer sex practices, such as using latex condoms, are effective in
preventing HIV transmission. But there is a risk of getting the
infection, even with the use of condoms. Abstinence is the only sure way
to prevent sexual transmission of HIV.
HIV-positive patients who are taking antiretroviral medicines are less
likely to transmit the virus.
The U.S. blood supply is among the safest in the world. Nearly all
people infected with HIV through blood transfusions received those
transfusions before 1985, the year HIV testing began for all donated
blood.
If you believe you have been exposed to HIV, seek medical attention
right away. Do not delay. Starting antiviral medicines can reduce the
chances that you will be infected. This is called post-exposure
prophylaxis (PEP). It has been used to prevent transmission in health
care workers injured by needle sticks
TREATMENT
There is no cure for AIDS at this time. But treatments are available to
manage symptoms. Treatment can also improve the quality and length of
life for those who have already developed symptoms.
Antiretroviral therapy suppresses the replication of the HIV virus in
the body. A combination of antiretroviral drugs, called antiretroviral
therapy (ART), also known as highly active antiretroviral therapy
(HAART), is very effective in reducing the amount of HIV in the
bloodstream. This is measured by the viral load (how much free virus is
found in the blood). Preventing the virus from reproducing (replicating)
can improve T-cell counts and help the immune system recover from HIV
infection.
People on ART with suppressed levels of HIV can still transmit the virus
to others through sex or by sharing needles. With ART, if the level of
HIV remains suppressed and CD4 count remains high (above 200 cells/mm3),
life can be prolonged and improved.
HIV can become resistant to one combination of ART. This is most true in
patients who do not take their medications on schedule every day. Tests
can check whether an HIV strain is resistant to a particular drug. This
information can be useful in finding the best drug combination and for
adjusting the drug combination when it starts to fail.
When HIV becomes resistant to HAART, other drug combinations must be
used to try to suppress the resistant HIV strain of HIV. There are a
variety of new drugs on the market for treating drug-resistant HIV.
Treatment with ART has complications. Each drug has its own side
effects. Common side effects are:
Collection of fat on the back (buffalo hump) and abdomen
Diarrhea
General sick feeling ( malaise)
Headache
Nausea
Weakness
When used for a long time, these drugs increase the risk of heart
attack, perhaps by increasing the levels of cholesterol and glucose
(sugar) in the blood.
TRENDS IN HIV CURE
One of the major limitations of ART is its inability to act on viral
reservoirs requiring adherence to lifelong treatment. HIV cure has been
currently the main focus area in HIV research to avoid toxicities and
cost of lifelong ART. Strategies attempted so far for HIV cure consist
of purging of HIV reservoir by activation in presence of anti-HIV drugs,
bone marrow transplantation and gene therapy [14]. Initiating ART early
during acute phase of the infection can also help to achieve functional
cure by limiting development of size of the viral reservoir. Recently
reported Mississippi case and a report on Visconti's cohort have
highlighted the benefits of the early treatment. Berlin and Boston cases
reporting HIV cure in cancer patients after bone marrow transplantation
along with the Mississipi case have helped in raising hopes for the HIV
cure.

A burn is damage to your body's tissues caused by heat, chemicals, electricity, sunlight or radiation. Scalds from hot liquids and steam, building fires and flammable liquids and gases are the most common causes of burns. Another kind is an inhalation injury, caused by breathing smoke.
There are three types of burns:
First-degree burns damage only the outer layer of skin
Second-degree burns damage the outer layer and the layer underneath
Third-degree burns damage or destroy the deepest layer of skin and tissues underneath
Burns can cause swelling, blistering, scarring and, in serious cases, shock and even death. They also can lead to infections because they damage your skin's protective barrier. Antibiotic creams can prevent or treat infections. After a third-degree burn, you need skin or synthetic grafts to cover exposed tissue and encourage new skin to grow. First- and second-degree burns usually heal without grafts.
Second-degree burns damage the outer layer and the layer underneath
Third-degree burns damage or destroy the deepest layer of skin and tissues underneath
Burns can cause swelling, blistering, scarring and, in serious cases, shock and even death. They also can lead to infections because they damage your skin's protective barrier. Antibiotic creams can prevent or treat infections. After a third-degree burn, you need skin or synthetic grafts to cover exposed tissue and encourage new skin to grow. First- and second-degree burns usually heal without grafts.
For minor burns, including first-degree burns and second-degree burns limited to an area no larger than 3 inches (7.6 centimeters) in diameter, take the following action:
- Cool the burn. Hold the burned area under cool (not cold) running water for 10 or 15 minutes or until the pain subsides. If this is impractical, immerse the burn in cool water or cool it with cold compresses. Cooling the burn reduces swelling by conducting heat away from the skin. Don't put ice on the burn.
- Cover the burn with a sterile gauze bandage. Don't use fluffy cotton, or other material that may get lint in the wound. Wrap the gauze loosely to avoid putting pressure on burned skin. Bandaging keeps air off the burn, reduces pain and protects blistered skin.
- Take an over-the-counter pain reliever. These include aspirin, ibuprofen (Advil, Motrin, others), naproxen (Aleve) or acetaminophen (Tylenol, others). Use caution when giving aspirin to children or teenagers. Though aspirin is approved for use in children older than age 2, children and teenagers recovering from chickenpox or flu-like symptoms should never take aspirin. Talk to your doctor if you have concerns.
For major burns, call emergency medical help. Until an emergency unit arrives, follow these steps:
- Don't remove burned clothing. However, do make sure the victim is no longer in contact with smoldering materials or exposed to smoke or heat.
- Don't immerse large severe burns in cold water. Doing so could cause a drop in body temperature (hypothermia) and deterioration of blood pressure and circulation (shock).
- Check for signs of circulation (breathing, coughing or movement). If there is no breathing or other sign of circulation, begin CPR.
- Elevate the burned body part or parts. Raise above heart level, when possible.
- Cover the area of the burn. Use a cool, moist, sterile bandage; clean, moist cloth; or moist cloth towels.
Caution
- Don't use ice. Putting ice directly on a burn can cause a person's body to become too cold and cause further damage to the wound.
- Don't apply egg whites, butter or ointments to the burn.This could cause infection.
- Don't break blisters. Broken blisters are more vulnerable to infection.

If you have diabetes, your blood glucose, or blood sugar, levels are too high. Over time, this can damage your nerves or blood vessels. Nerve damage from diabetes can cause you to lose feeling in your feet. You may not feel a cut, a blister or a sore. Foot injuries such as these can cause ulcers and infections. Serious cases may even lead to amputation. Damage to the blood vessels can also mean that your feet do not get enough blood and oxygen. It is harder for your foot to heal, if you do get a sore or infection.
You can help avoid foot problems. First, control your blood sugar levels. Good foot hygiene is also crucial:
Check your feet every day
Wash your feet every day
Keep the skin soft and smooth
Smooth corns and calluses gently
If you can see, reach, and feel your feet, trim your toenails regularly. If you cannot, ask a foot doctor (podiatrist) to trim them for you.
Wear shoes and socks at all times
Protect your feet from hot and cold
Keep the blood flowing to your feet

OverviewBirth-acquired herpes is a herpes virus infectionthat an infant gets (acquires) at the time of birth.Newborn infants can become infected with herpesvirus:-- In the uterus (intrauterine herpes -- this is veryrare) 1
Overview-- Passing through the birth canal (birth-acquiredherpes, the most common method of infection)-- Right after birth (postpartum) from kissing orhaving other contact with someone who hasherpes mouth sores 2
OverviewIf the mother has an active genital herpes infectionat the time of delivery, the baby is more likely tobecome infected during birth. Some mothers maynot be aware they have internal (inside the vagina)herpes sores.Some people have had herpes infections in thepast, but were not aware of it. These people, notknowing that they have herpes, may pass it to theirbaby. 3
OverviewHerpes type 2 (genital herpes) is the most commoncause of herpes infection in newborn babies, butherpes type 1 (oral herpes) can also occur.Medline Plus - National Institutes of Health: 4
SymptomsHerpes may only appear as a skin infection.Small, fluid-filled blisters (vesicles) may appear.These blisters rupture, crust over, and finallyheal, often leaving a mild scar.Herpes infection may also spread throughout thebody (called disseminated herpes). In this type, theherpes virus can affect many different parts of thebody. 5
Symptoms-- Herpes infection in the brain is called herpesencephalitis-- The liver, lungs, and kidneys may also beinvolved-- There may or may not be blisters on the skin 6
SymptomsNewborn infants with herpes that has spread tothe brain or other parts of the body are often verysick. Symptoms include: 7
TreatmentHerpes virus infections in infants are generallytreated with medicine given through a vein(intravenous). Acyclovir is the most commonantiviral medicine used for this purpose. The babymay need to take the medicine for several weeks. 8
TreatmentOther therapy is often needed to treat the effectsof herpes infection, such as shock or seizures.Often, because these babies are very ill, treatmentis done in an intensive care unit.Herpes virus infections in infants are generallytreated with medicine given through a vein(intravenous). Acyclovir is the most commonantiviral medicine used for this purpose. The babymay need to take the medicine for several weeks. 9
TreatmentOther therapy is often needed to treat the effectsof herpes infection, such as shock or seizures.Often, because these babies are very ill, treatmentis done in an intensive care unit. 10
Diagnosis **When to Contact a Medical Professional**If your baby has any symptoms of birth-acquiredherpes, including skin lesions alone, have the babyseen by your health care provider promptly.Medline Plus - National Institutes of Health: 11
RisksPossible Complications:-- Bacterial or fungal infection of skin lesions-- Coma-- Death-- Developmental delay 12
Risks-- Excessive bleeding, disseminated intravascularcoagulation (DIC)-- Eye problems (chorioretinitis, keratitis)-- Gastrointestinal problems, including diarrhea-- Hepatitis-- Jaundice 13
Risks-- Liver failure-- Lung problems including pneumonia orpneumonitis-- Brain and nervous system (neurological)problems-- Respiratory distress-- Seizure 14
Risks-- Shock-- Skin lesionsMedline Plus - National Institutes of Health: 15
Riskshttp://www.nlm.nih.gov/medlineplus/ency/article/001368.htm 16
PreventionIt is important for women to tell their doctor ifthey have a history of genital herpes.Safer sexual practices can help prevent the motherfrom getting genital herpes. Mothers who are notinfected with herpes cannot pass the herpes virusto the baby during delivery. 17
PreventionPeople with "cold sores" (herpes labialis) shouldavoid contact with newborn infants. Caregiverswho have a cold sore should wear a surgical maskand wash their hands carefully before coming intocontact with the infant to prevent transmitting thevirus.Mothers should speak to their health careproviders about the best way to minimize the riskof transmitting herpes to their infant.

Mouth ulcers are sores that appear in the mouth, often on the inside of the cheeks.
Mouth ulcers, also known as apthous ulcers, can be painful when eating, drinking or brushing teeth.
Occasional mouth ulcers are usually harmless and clear up on their own. Seek medical advice if they last longer than 3 weeks or keep coming back.
Mouth ulcers cannot be caught from someone else.
Up to 1 in 5 people get recurrent mouth ulcers.
Canker sores (also called aphthous ulcers).
Types of mouth ulcer
The main types of mouth ulcer are:
Minor ulcers. These are around 2-8mm in diameter and usually clear up in 10 days to 2 weeks.
Major ulcers. These are bigger and deeper, often with a raised or irregular border. This type of ulcer can take several weeks to heal and may leave a scar in the mouth.
Herpetiform ulcers: This type of ulcer is a cluster of dozens of smaller sores the size of pinheads.
What causes mouth ulcers?
The exact cause of most mouth ulcers is unknown. Stress or tissue injury is thought to be the cause of simple mouth ulcers. Certain foods, including citrus or acidic fruits and vegetables (such as lemons, oranges, pineapples, apples, figs, tomatoes and strawberries), can trigger a mouth ulcer or make the problem worse. Sometimes a sharp tooth surface or dental appliance, such as braces or ill-fitting dentures, might also trigger mouth ulcers.
Some cases of complex mouth ulcers are caused by an underlying health condition, such as an impaired immune system; nutritional problems, such as vitamin B-12, zinc, folic acid, or iron deficiency and gastrointestinal tract disease, such as Coeliac disease and Crohn's disease.
When you first quit smoking, you may develop more mouth ulcers than normal, but this is temporary.
Some medications, including common pain killers, beta-blockers and some chest pain medicines may cause a reaction that leads to mouth ulcers.
What are the symptoms of mouth ulcers?
You may have a mouth ulcer if you have:
A painful sore or sores inside your mouth, on the tongue, soft palate (the back portion of the roof of your mouth), or inside your cheeks.
Sores in your mouth that are round, white, or grey in colour, with a red edge or border.
In severe mouth ulcer attacks, you may also experience:
Fever
Physical sluggishness
Swollen lymph nodes
How are mouth ulcers treated?
Pain from a mouth ulcer generally lessens in a few days and the sores usually heal without treatment in about a week or two.
If sores are large, painful or persistent, your dentist may prescribe an antimicrobial mouth rinse, a corticosteroid ointment, or a prescription or non-prescription solution to reduce the pain and irritation.
Can mouth ulcers be prevented?
Although there is no cure for mouth ulcers and they often reoccur, you may be able to reduce their frequency with good dental hygiene and by:
Avoiding foods that irritate your mouth, including acidic or spicy foods
Avoiding irritation from gum chewing
Brushing with a soft-bristled brush after meals and flossing daily, which will keep your mouth free of foods that might trigger a sore.
Seek medical advice about mouth ulcers if you have:
Unusually large sores
Sores that are spreading
Sores that last three weeks or longer
Intolerable pain despite avoiding trigger foods and taking over-the-counter pain medication
Difficulty drinking enough fluids
A high fever with the appearance of the mouth ulcer(s)

New research published in The Lancet by researchers from the Harvard School of Public Health (HSPH) and the Icahn School of Medicine at Mount Sinai (ISMMS) found that various chemicals that many children are exposed to are having a direct effect on the creation of disorders labelled under the name ADHD as well as other mental disorders. One of the chemicals said to be having an effect is fluoride, or variations of fluoride. Governments have been performing artificial fluoridation for a number of years regardless of the lack of effectiveness it has in preventing tooth decay. The research began in a study published in 2006 which initially looked at the effects of various industrial chemicals on neuro-development.[1] The research continued with an analysis of more industrial chemicals including fluoride. 27 additional studies, including one that linked fluoride to the lowering of IQ in children, clearly illustrated the fact that fluoride is detrimental to brain development and can lead to autism spectrum disorders and other mental issues. The issue is being coined “a silent epidemic” and most health authorities continue to turn a blind eye to the issue. The two main researchers involved in the study, Philippe Grandjean from HSPH and Philip Landrigan, both agree that the reason for the increase in incidences of chemical-related neuro-developmental disorders is due to the increasing number of untested chemicals that are being approved without proper testing. The public is also not fully being told of the dangers which is causing many to perform independent research to find out the true effects. The issue is not just in water fluoridation, but also in the vaccination of our children. “Since 2006, the number of chemicals known to damage the human brain more generally, but that are not regulated to protect children's health, had increased from 202 to 214,” writes Julia Medew for The Sydney Morning Herald. “The pair said this could be the tip of the iceberg because the vast majority of the more than 80,000 industrial chemicals widely used in the United States have never been tested for their toxic effects on the developing fetus or child.” The fact is, fluoride is a known developmental neurotoxin and practices of water fluoridation have long been proven to be ineffective. If individuals choose to use fluoridated tooth paste or choose fluoride treatments at their dental office, that is acceptable but two things should happen: 1. People should be taught about the harmful effects of fluoride and the damage it can cause to your teeth and your body. 2. Water fluoridation should be stopped everywhere immediately as it is nothing more than a legal way for chemical companies to get rid of toxic waste while profiting. Fluoride accumulates in the body over time, so even though the amounts being ingested might be small each time, it builds up over years and can cause serious health issues. Research has found that fluoride affects normal endocrine function, causes kidney disease, bone weakness, dental fluorosis, cancer, lowering of IQ, calcification of the pineal gland, arthritis, immune deficiencies, skeletal fluorosis and much more. “The problem is international in scope, and the solution must therefore also be international,” stated Grandjean in a press release, calling for improved regulatory standards for common chemicals. “We have the methods in place to test industrial chemicals for harmful effects on children's brain development — now is the time to make that testing mandatory.

INTRODUCTION
Tobacco smoking is a significant risk factor for periodontal disease Environmental &acquired risk factors [SMOKING] Ag Specific LPS pathogenic bacteria Ab Cytokines,PGE2 Host Connective immune tissue & inflambone MMPs matory metabolism response PMNs Genetic risk factors Clinical expression of disease, initiation progression
EPIDEMIOLOGICAL EVIDENCE
• Cross-sectional and case-control studies demonstrate a moderate to strong association between smoking and periodontitis*Hill’s criteria+. • Smokers are 4x as likely to develop periodontitis as non-smokers. • Smoking may be responsible for more than half of the periodontal disease among adults. • Up to 90% of refractory periodontitis patients are smokers. (MacFarlane et al, 1992)
RISK ASSESSMENT ATTACHMENT LOSS
Variable Estimated odds ratio Age 1.72 - 9.01 Smoking 2.05 - 4.75 Diabetes 2.32 P gingivalis 1.59 Education 0.65 (Grossi et al, 1994)
ATTACHMENT LOSS AND SMOKING 40 30 20 10 0 Pack years healthy low moderate high (Grossi et al, 1994) severe
10 year prospective study of smoking and periodontitis [Bergstrom et al 2000] Smokers lost significantly more periodontal bone compared to nonsmokers (p<0.001)
AGE, SEX, AND CIGARETTE SMOKING
Carranza stated women from ages 20 to 39 and men from ages 30 to 59 who smoke cigarettes have twice the chance of having periodontal disease or becoming edentulous as do non-smokers The effects of smoking on periodontal status to be more pronounced in younger women. [Goultschin et al.10]
PREVALENCE OF MODERATE AND SEVERE PERIODONTITIS
• Current smokers - 25.7% • Former heavy smokers - 20.2% • Cigar/pipe smokers - 17.6% • Non-smokers - 13.1% [ Albandar et al 2000]
Stopping smoking (for 10 years) reduces risk of periodontitis to that of non-smokers 0-2 years -> OR=3.2 >10 years -> OR=1.2 The more you smoke the worse the periodontitis (dose response) Smoking <10 cigs/day OR = 2.8 Smoking >30 cigs/day OR = 6.9 [Tomar and Asma 2000]
Tobacco contains over 4,000chemicals, many of which are harmful. These include: Benzene - solvent used in fuel manufacture Formaldehyde - highly poisonous, colourless liquid used to preserve dead bodies Ammonia - chemical found in cleaning fluids. Used in cigarettes to increase the delivery of nicotine Hydrogen cyanide -poisonous gas used in the manufacture of plastics, dyes, and pesticides. - Often used as a fumigant to kill rats Cadmium - extremely poisonous metal found in batteries Acetone - solvent found in nail polish remover
POTENT CARCINOGENS
• Nitrosamines • Polycyclic aromatic hydrocarbons • Radiation-emitting polonium COMPONENTS OF INHALED SMOKE •Nicotine •Carbon monoxide •Tar all of which can cause disease
Nicotine action • Accelerates release of neurotransmitter dopamine in the brain’s NA* & increases metabolism in NA *NA = nucleus accumbens
•Nicotine retards growth of gingival fibroblasts reduces fibronectin & collagen increases collagen breakdown Other actions are: •raise blood pressure •stimulants •vasoconstriction •psychological - social dependency •physical dependancy - craving
CARBON MONOXIDE-ACTIONS
•Carbon monoxide is a poisonous gas found in car fumes, which reduces the amount of oxygen carried in the blood. •Oxygen is vital for the body’s organs to function efficiently. • The reduction in oxygen changes the consistency of the blood, making it thicker and putting the heart under increased strain as it pumps blood around the body
TAR-actions •Tar contains many substances proven to cause cancer. •Irritants found in tar damage the lungs causing narrowing of the tubes(bronchioles) and damaging the small hairs (cilia) that protect the lungs from dirt and infection
Effect of Smoking on Plaque
PERIODONTAL PATHOGENS
The proportions of subjects positive for A. actinomycetemcommitans, P. gingivalis, and T. forsythesis were higher among smokers. {Zambon et al.(1996),using a fluorescence technique in a Cross sectional study from Erie County Study population} Furthermore, increased counts of exogenous flora (Escheria coli and Candida albicans) have been reported in smokers
SMOKING AND HOST RESPONSE
• Smoking decreases salivary IgA and serum IgG,and specifically reduces IgG2 levels against A.a.commitans (Bennet & Read, 82; Barbour et al.,97). • The ability of tobacco products to decrease the proliferating capacity of T and B lymphocytes might contribute to this diminished production of protective antibodies.
• Smoking can exert deleterious effects on polymorphonuclear leukocytes (PMN) and other neutrophil functions such as chemotaxis & phagocytosis so that they cannot efficiently deal with the bacterial infection (Kenney et al., 1977; Eichel & Shahrik, 1969; Selby et al., 1992). • Impaired phagocytosis function of neutrophils among smokers with refractory periodontitis. (MacFarlane et al., 1992).
In addition, tobacco smoking may modify the production of pro-inflammatory cytokines IL-1 and TNF-ᾳ which are considered key regulators of the host response to microbial challenge. ( Kornman et al. ,1997)
Genetic Polymorphism and Smoking Investigators have looked at genetic variability, its relationship with periodontal disease, and its interaction with smoking. Tooth loss reported a positive genotype of IL-1 increases the risk for tooth loss by 2.7 times, while smoking increases the risk by 2.9 times. When both were combined, the risk increased to 7.7 times.*JCDP’08+
EFFECT OF SMOKING ON GINGIVA
Cigarette Smoking and Gingival Bleeding Smokers expressed less gingival bleeding than non-smokers
This is also proved to be dose dependant
This may be due to vasoconstrictive effect of nicotine. Clarke et al 1984
Effect of Smoking on Gingival Blood Flow • In smokers, gingival blood flow was significantly increased by cigarette smoking. • However, intravenous administration of nicotine reduces the marginal temperature of gingival sites suggesting a decrease in gingival blood flow which lead to the hypothesis this phenomenon is caused by vasoconstriction induced by nicotine and stress
Oxygen Tension in the Gingival Tissues • Smoking Decreases Tissue Oxygen • Tissue oxygen decreases: 65 ± 7 to 44 ± 3 mmHg [Jensen, et al. Arch Surg, 1991] • Tissue oxygen 40-50 mmHg —> infection Effects on the Gingival Vasculature researchers found a high proportion of small vessels compared with large vessels in smokers than non-smokers but no difference in the vasculature density. [journal CDP nov08]
Evidence From Studies on (GCF) Smoking may result in lower resting GCF flow rate. The increase in GCF during an experimental gingivitis may be less in smokers. Studies have shown higher levels of TNF-α and decreased levels of IL-1α and IL-1β ,enzyme elastase in GCF when compared between smokers and nonsmokers. This research has demonstrated there are lower levels of cytokines, enzymes, and possibly polymorphonuclear leukocytes (PMNs). This correlates with the lower levels of inflammation observed clinically and within the tissues. Kinane and Radvar 1997
Smoking and Fibroblast Function Gingival Fibroblasts In vitro studies have shown reduction in the production of Type 1 collagen and fibronectin and an increase in the collagenase activity. Cellular changes like disruption of cell orientation, changes in cytoskeleton, presence of large vacuoles, and significant reduction in cell viability have been noticed.
Smoking and gingival inflammation Smokers may present with lower levels of gingival inflammation than nonsmokers. Furthermore, development of gingival inflammation in response to experimental plaque accumulation (experimental gingivitis) was less pronounced in smokers than in non-smokers. [Albander et al 99, Lie et al 98]
Periodontal fibroblast
PDL fibroblast growth, attachment and integrin expression was inhibited by nicotine at high concentrations (≥1 mg/ml)
Nicotine at high concentrations (100 ng/ml to 25μg/ml) to be cytotoxic by inhibiting the vacuolation and proliferation of fibroblasts. [Giannopovlou et al.27]
PDL cell proliferation and protein synthesis were also inhibited in a dose dependent manner.
Cell attachment was significantly less on root surfaces obtained from heavy smokers compared with nonsmokers.
Smoking and periodontitis in young adults (≤35 years) Several studies have shown young adult smokers aged 19-30 years had a higher prevalence and severity of periodontitis compared to non-smokers despite similar or lower plaque levels. The prevalence of periodontitis, defined as having a site with attachment loss of ≥2 mm and probing depths of ≥4 mm, was three to four times higher in young smokers compared to non-smokers. [Haber et al]
Smoking and Periodontitis in Adults Current smokers have deeper probing depths, greater attachment loss, more bone loss, and fewer teeth. Smokers also exhibit more supragingival calculus deposits. Smokers were four times more likely to have periodontitis as compared to non-smokers.
Among 20-49 year-olds, the adjusted odds ratio for a mean attachment loss of 1 to 1.99 mm among current smokers was 2.29, whereas the odds ratio for attachment loss ≥3 mm was over 18.43. This suggests smoking is particularly important in the etiology of severe periodontal attachment loss. {NHANES}
There is a strong dose-response relationship between the amount smoked and the severity of periodontal destruction which further supports the role of smoking as a risk factor for periodontitis. The most marked difference between smokers and non-smokers in probing depths or attachment loss occurs in the maxillary lingual area and mandibular anterior area, suggesting a local effect of smoking.
Effects of Smokeless Tobacco on Periodontal Tissues
It involves chewing a quid that includes betel leaf,lime, areca nut, and tobacco.
Tobacco use may significantly increase bleeding on probing and periodontal attachment loss.
Other studies have also shown the negative effect of the areca nut on host immunity by affecting PMNs.
Arecanut extracts have also been shown to inhibit the growth, attachment, and matrix protein synthesis of cultured human gingival fibroblasts.
Smoking and Acute Necrotizing Ulcerative Gingivitis (ANUG) An association between necrotizing forms of periodontal disease and tobacco smoking was reported as early as 1947 Preexisting gingivitis, emotional/psychic stress, and smoking forms a triad of interrelated predisposing factors in the etiology of the disease. .
SMOKING influence the tissue response to irritation. activates the release of epinephrine promotes contraction of peripheral vessels reducing blood flow to the gingiva loss of vitality to the gingival epithelium onset of ANUG .{Karadachi et al}
SMOKING AND SYSTEMIC HEALTH
Smoking and cardiovascular system •Smoking causes coronary heart disease, atherosclerosis, arteriosclerosis, heart attack the leading cause of death •Cigarette smoking causes reduced circulation by narrowing the blood vessels (arteries) and puts smokers at risk of developing peripheral vascular disease •Smoking causes abdominal aortic aneurysm (i.e., a swelling or weakening of the main artery of the body—the aorta—where it runs through the abdomen).Smoking and Respiratory Disease Smoking causes lung cancer. Smoking causes lung diseases (e.g., emphysema, bronchitis, chronic airway obstruction) by damaging the airways and alveoli (i.e., small air sacs) of the lungs. Smoking and brain Can cause stroke which may be fatal or cause mental and physical disability
Smoking and Cancer Smoking causes the following cancers:1 *Acute myeloid leukemia *Bladder cancer *Cancer of the cervix *Cancer of the esophagus *Kidney cancer *Cancer of the larynx (voice box) *Lung cancer *Cancer of the oral cavity (mouth) *Pancreatic cancer *Cancer of the pharynx (throat) *Stomach cancer
Smoking and Other Health Effects Smoking has many adverse reproductive and early childhood effects, including increased risk for— infertility, preterm delivery, stillbirth, low birth weight, and sudden infant death syndrome (SIDS). Smoking is associated with the following adverse health effects: Postmenopausal women who smoke have lower bone density than women who never smoked.
SMOKING – MORBIDITY
(miller et al 1999) 50% of total cancer deaths 84% of lung cancer deaths 30% of heart disease deaths 23% of respiratory deaths 80% of bronchitis and emphysema deaths
Interaction between smoking and systemic Health status and periodontitis The combination of smoking with other systemic factors further enhances the risk of periodontal destruction. .
•Studies say that the combination of diabetes and heavy smoking in an individual over the age of 45 years who harbored P. gingivalis or T. forsythesis resulted in an odds ratio of attachment loss 30 times that of a person lacking these risk factors.(JCDP nov,2008) •Smoking also increases the risk of attachment and/or bone loss in AIDS and HIV serotype patients. •Periodontitis also may worsen the systemic status of an individual
SMOKING AND ORAL HEALTH
Tobacco use in all forms, especially cigarette smoking, is the number one risk factor for oral cancer. Possible mechanisms are •Irritants and toxic substances in tobacco •Change in Ph •Change in immune response •Dryness due to heat produced while smoking The most common form of cancer is Squamous cell carcinoma. •The most common sites of the oral cancer is the tongue and the floor of the mouth. • The other common sites are buccal vestibule, buccal mucosa, gingiva and rarely hard and soft palate. • Cancer of bucco-pharyngeal mucosa is common in smokers.Abnormal Changes at Cancerization site • Clinically: – Leukoplakia – Erythroplasia – Dysplasia – Carcinoma in situ
OTHER LESIONS: SMOKER’S PALATE
• Palate becomes white with tiny red spots-raised duct opening of salivary glands [dried mud appearance]

SMOKER’S MELANOSIS
• Brown spots on oral mucosa HAIRY TONGUE • Overgrowth of papilla on the surface of tongue COATED TONGUE • Tongue coated with food particles, bacteria and debris from epithelium
DENTAL CARIES AND EROSION
• Smoking stimulates saliva flow immediately, does not affect saliva in long term • Decrease Ph and buffering action Dental caries Erosion GINGIVAL RECESSION
• STAINING OF TEETH • HALITOSIS • DELAYED WOUND HEALING • DRY SOCKET • SMOKER’S FACE
Effects Of Smoking On Periodontal Therapy
CIGARETTE SMOKING AND ORAL HYGIENE
Several studies demonstrated higher levels of oral debris in smokers than in non-smokers. Increased levels of debris observed in smokers have been tentatively attributed to personality traits leading to decreased oral hygiene habits, increased rates of plaque formation, or a combination of the above. *JCDP’08+
Toothbrushing efficiency of smokers was much less and the calcium concentration in the dental plaque of smokers was found to be significantly higher than in nonsmokers. [Medicine and Biology Vol.14, No 2, 2007, pp. 53 – 59]
EFFECT OF SMOKING IN WOUND HEALING
Smoking has been shown to impair revascularization during soft and hard tissue wound healing, which is critical for periodontal plastic, regenerative, and implant procedures. (Nolan et al.,85; Preber & Bergström, 85a; 86; 90).
Non-surgical and Surgical Therapy Numerous studies have shown smoking compromises probing depth and/or attachment gain outcomes following non-surgical or surgical therapy. The numerical differences between smokers and non-smokers become more pronounced in probing depths ≥5 mm, where smokers demonstrated 0.4 mm to 0.6 mm less improvement in clinical attachment levels following scaling and root planning. Following flap debridement surgery, smokers experienced upto 1 mm less improvement in clinical attachment levels in probing depths that were initially ≥7mm.
Antimicrobial Therapy in Smokers • Because of the diminished treatment response insmokers, clinicians may recommend adjunctive antimicrobial therapy for smokers. • Because subgingival pathogens are more difficult to eliminate in smokers following SRP. • Systemic amoxicillin and metronidazole or locally delivered minocycline microspheres enhanced the results of mechanical therapy. • A recent study reported a positive response to subantimicrobial doxycycline (anticollagenase) therapy in combination with SRP in a group of severe periodontitis patients that included smokers.
Soft and Hard Tissue Grafting • In guided tissue regeneration procedures smokers had significantly less root coverage(57%) compared to nonsmokers (78%) • Smoking is detrimental to regenerative therapy in interproximal and furcation defects, whether treatment includes the use of osseous graft, bioabsorbable membrane, or a combination. • The results have shown less than 50% as much improvement in clinical attachment levels in smokers, which amounted to differences ranging from 0.35 mm to 2.9 mm.
Implant Therapy • In the studies reviewed, 0% to 17% of implants placed in smokers were reported as failures as compared to 2% to 7% in non-smokers. • The 3-year data demonstrated 8.9% of implants placed in smokers failed as compared to 6% in individuals who had never smoked or had quit smoking. • The majority of implant failures in smoking occurred prior to prosthesis delivery.
Maintenance phase • ↑pocket depth • ↓gain in clinical attachment level • Deeper and more residual pockets after flap surgery Refractory disease • ↑recurrence and ↑need for re treatment and antibiotic therapy • ↑tooth loss after surgical therapy
TOBACCO CESSATION
64The “5 A’s” To Intervention • ASK about tobacco use. • ADVISE to quit. • ASSESS willingness to make a quit attempt. • ASSIST in quit attempt. • ARRANGE for followup.
Nicotine withdrawal: the 4 ‘D’s Drink water slowly Deep breathe. Do something else (eg exercise) Delay acting on the urge to smoke
PHARMACOTHERAPY Pharmacotherapy + behavioural counselling improves long-term quit rates Smokers of 10 or more cigarettes a day who are ready to stop should be encouraged to use pharmacologial support as a cessation aid Nicotine replacement • Begin NRT on the quit date, (apply patches the night before) • Use a dose that controls the withdrawal symptoms • NRT provides levels of nicotine well below smoking • Prescribe in blocks of two weeks • Arrange follow up to provide support • Use a full dose for 6 to 8 weeks then stop
NRT: Nicotine patches • • • Patches provide a slow, consistent release of nicotine throughout the day Available in various shapes and sizes, Common side effects with patches include skin sensitivity and irritation NRT: Nicotine nasal sp • • Nasal sprays more closely mimic nicotine from cigarettes Common side effects with nasal sprays include nasal and throat irritation, coughing and oral burning NRT: Nicotine gum • • • • Instruct the patient to ‘chew and park’ Absorption may be impaired by coffee and some acidic drinks Common side effects with gum include gastrointestinal disturbances and jaw pain Dentures may be a problem!
Nicotine Tabs • • Nicotine tablets deliver 2-mg or 4-mg dosages of nicotine over 30-minutes Common side effects with gum include burning sensations in the mouth, sore throat, coughing, dry lips, and mouth ulcers Bupropion • Begin bupropion a week before the quit date • Normal dose 150mg bd, (reduce in elderly, liver/renal disease) • Contra-indicated in patients with epilepsy, anorexia nervosa, bulimia, bipolar disorder or severe liver disease. • The most common side effects are insomnia (up to 30%), dry mouth (10-15%), headache (10%), nausea (10%), constipation (10%), and agitation (5-10%) • Interaction with antidepressants, antipsychotics and antiarrhythmics • Nicotine replacement and buproprion should always be used in conjunction with behavior modification
Nortryptiline • Tri-cyclic antidepressant • Not licensed for smoking cessation • Low cost • Side-effects include sedation, dry mouth, light-headedness, cardiac arrhythmia • Contra-indicated after recent myocardial infarction Varenicline • Begin varenicline a week before the quit date, increasing dose gradually. • Alleviates withdrawal symptoms, reduces urge to smoke • Common side effects include: nausea (30%), insomnia, (14%), abnormal dreams (13%), headache (13%), constipation (9%), gas (6%) and vomiting (5%). • Contra-indicated in pregnancy
Smokers may move backwards or forwards, to and fro across the cycle many times before finally quitting Relapse Precontemplation Maintenance Cycle of change Action Contemplation Determination
Impact of Smoking Cessation on Periodontal Status and Treatment Outcomes •While smoking cessation does not reverse the past effects of smoking, the rate of bone and attachment loss slows after patients quit smoking and the severity of their disease is intermediate compared to current and non-smokers. •It is encouraging to note former smokers respond to non-surgical and surgical therapy in a manner similar to nonsmokers. •Similarly, implant success rates for past smokers were similar to nonsmokers.(JCDP’08)
CONCLUSION
It is clear that smokers • Present with periodontitis at an early age • Difficult to treat them with conventional therapy • Continue to have progressive or recurrence of periodontitis leading to tooth loss The opportunity for dentists to become more active in evaluation of tobacco use by patients and more aggressive in offering counseling and cessation services can positively impact both the oral and general health of dental patients.

DESQUAMATIVE GINGIVITIS Chronic desquamative gingivitis was first recognized and reported in 1894. In 1932, Prinz described it as a peculiar condition characterized by intense erythema, desquamation and ulceration of the free and attached gingiva. Patients may be asymptomatic,however when symptomatic, their complaints range from a mild sensation to an intense pain. Etiology is unknown. 50% of desquamative gingivitis cases are localized to gingiva, although involvement of intraoral and extra oral sites is not uncommon. Diagnosed in women in the fourth to fifth decades of life (may occur as early as puberty or as late as seventh or eighth decades). In 1960 McCarthy and colleagues suggested that desquamative gingivitis was not a specific disease entity, but a gingival response associated with a variety of conditions.
There may be threads or loose necrotic epithelium. It involves not only marginal gingiva, but also peels the attached gingiva often in a band- like fashion. The differential diagnosis of desquamative gingivitis include a variety of diseases such as lichen planus, cicatrical pemphigoid, bullous pemphigoid, pemphigus vulgaris,linear IgA disease, dermatitis herpetiformis and drug reaction or eruptions. DIAGNOSIS : The success of any given therapeutic approach resides on the establishment of an accurate final diagnosis.
CLINICAL FEATURES : Mild form. Moderate form. Severe form.
MILD FORM : There is diffuse erythema of the marginal, interdental and attached gingiva. It is usually painless and occurs most frequently in females between 17 & 23yrs. of age.
MODERATE FORM : Patchy distribution of bright- red and gray areas involving marginal and attached gingiva. The surface is smooth and shiny, normal resilient gingiva becomes soft, edematous and massaging of gingiva results in peeling off the epithelium. Usually seen in the age group of 30 to 40 yrs. Patient complains of burning sensation. The labial surface is more frequently involved.
SEVERE FORMS : This form is characterized by scattered irregularly- shaped areas in which the gingiva is denuded and strikingly red in appearance. The gingiva is speckled and the surface epithelium seem shredded, friable and can be peeled off in small patches. The mucous membrane other than gingiva is smooth and shiny and may present fissuring in the cheek adjacent to the line of occlusion. The condition is painful. There is a constant, dry, burning sensation throughout the oral cavity.
HISTOPATHOLOGY : Microscopically, desquamative gingivitis often appears as bullous lesions or lichenoid lesions. Occasionally there will be thin , atrophic epithelium with little or no keratin at the surface and a dense, diffuse infiltration of chronic inflammatory cells in the underlying connective tissue.
Histochemical and ultastructural studies revealed separation of collagen fibrils and a decrease in the number of anchoring fibrils. THERAPY : It can be of two phases : Local Treatment. Systemic Treatment. LOCAL TREATMENT : Oral hygiene instructions (soft toothbrush). Oxidizing mouthwashes (Hydrogen peroxide 3% diluted). Topical corticosteroid ointments or cream- like triamcinolone 0.1%, flucocinamide 0.05%, desonide 0.05 %.
SYSTEMIC TREATMENT : Systemic corticosteroids in moderate doses. Prednisolone can be used in a daily or every- other- day dose of 30 - 40 mg and gradually- reduced to a daily maintenance dose of 5 – 10 mg.

HYPERTENSION
DEFINITION :
DEFINITION Hypertension (high BP) is a disease of vascular regulation in which the mechanisms that control arterial pressure within the normal range are altered. Predominant mechanisms of control are the central nervous system (CNS), the renal pressor system (renin-angiotensin-aldosterone system), and extracellular fluid volume.
TYPES OF HYPERTENSION :
TYPES OF HYPERTENSION PRIMARY HYPERTENSION SECONDARY HYPERTENSION ACCELERATED HYPERTENSION
CLASSIFICATION OF BLOOD PRESSURE FOR ADULTS :
CLASSIFICATION OF BLOOD PRESSURE FOR ADULTS
PRIMARY HYPERTENSION :
PRIMARY HYPERTENSION Also called as Essential Hypertension Approx. 95% of patients Diastolic -- 90 mm of Hg Systolic -- 140 mm of Hg or more
CAUSES :
CAUSES Idiopathic Hyperactivity of sympathetic vasoconstricting nerves Presence of vasoactive substance on smooth muscle Increased cardiac output, followed by arteriole constriction Excessive dietary sodium intake, sodium retention, insulin resistance, and hyperinsulinemia Familial (genetic) tendency
ISOLATED SYSTOLIC HYPERTENSION :
ISOLATED SYSTOLIC HYPERTENSION Systolic BP elevation in the absence of elevated diastolic BP is termed isolated systolic hypertension
SECONDARY HYPERTENSION :
SECONDARY HYPERTENSION Occurs in approx. 5% of patients with hypertension Renal pathology: Congenital anomalies, pyelonephritis, renal artery obstruction, acute and chronic glomerulonephritis Reduced blood flow to kidney causes release of renin. Renin reacts with serum protein in liver Coarctation of aorta Endocrine disturbances: Pheochromocytoma Adrenal cortex tumors Cushing’s syndrome Hyperthyroidism Medications such as estrogens, sympathomimetics, antidepressants, NSAIDs, steroids
Consequences of Hypertension :
Consequences of Hypertension Prolonged hypertension damages blood vessels in the brain, eyes, heart, and kidneys and increases the risk of stroke, angina, MI, blindness, and heart and kidney failure Blood vessel damage occurs through arteriosclerosis in which smooth muscle cell proliferation, lipid infiltration, and calcium accumulation occur in the vascular epithelium Damage to heart, brain, eyes, and kidneys is termed target organ disease; this is the major object of prevention in patients with high BP
Risk Factors :
Risk Factors Increase in incidence is associated with the following risk factors :- Age:- between 30 and 70 Race:- Black Overweight, sleep apnea Family history Smoking Sedentary lifestyle Diabetes mellitus Metabolic syndrome
RESEARCH EVIDENCE :
RESEARCH EVIDENCE Prevalence Black -30% Non-hispanic whites-25% Mexicans-Americans-22% Recent data have shown that only 70% of adults with hypertension are aware of it, 59% receive treatment, and only 34% reach BP control (less than 140/90 mm Hg).
CLINICAL MANIFESTATIONS :
CLINICAL MANIFESTATIONS Usually asymptomatic May cause headache, dizziness, blurred vision when greatly elevated BP readings more than 140/90 mm of Hg
DIAGNOSTIC EVALUATION :
DIAGNOSTIC EVALUATION ECG Chest X-ray Proteinuria, elevated serum blood urea nitrogen (BUN), and creatinine levels Serum potassium Urine (24-hour) for catecholamines Renal scan Renal duplex imaging Outpatient ambulatory BP measurements
MANAGEMENT(lifestyle modifications) :
MANAGEMENT(lifestyle modifications) Lose weight if body mass index is greater than or equal to 25. Limit alcohol Get regular aerobic exercise equivalent to 30 to 45 minutes of brisk walking most days. Cut sodium intake to 2.4 g or less per day Include recommended daily allowances of potassium, calcium, and magnesium in diet. Smoking cessation Reduce dietary saturated fat and cholesterol Consider reducing coffee intake
CONTD… :
CONTD… If, despite lifestyle changes, the BP remains at or above 140/90 mm Hg over 3 to 6 months, drug therapy should be initiated If BP extremely elevated or in presence of cardiovascular risk factors, single drug therapy may be given
CONSIDERATIONS IN SELECTING THERAPY :
CONSIDERATIONS IN SELECTING THERAPY Race:- Blacks respond well to diuretic therapy; Whites respond well to ACE inhibitors Age:- some adverse effects may not be tolerated well by elderly people Concomitant diseases and therapies:- some agents also treat migraines, benign prostatic hyperplasia, heart failure Quality of life impact:- tolerance of adverse effects Economic considerations:- newer agents very expensive
ANTI-HYPERTENSIVE DRUG GROUPS :
ANTI-HYPERTENSIVE DRUG GROUPS Diuretics Beta-adrenergic blockers Alpha-receptor blockers Central alpha agonists Peripheral adrenergic agents Combined alpha and beta-adrenergic blockers ACE inhibitors Angiotensin receptor blockers Calcium antagonists Direct vasodilators
BEST MANAGEMENT OF HYPERTENSION :
BEST MANAGEMENT OF HYPERTENSION To use the fewest drugs at the lowest doses while encouraging the patient to maintain lifestyle changes. After BP has been under control for at least 1 year, a slow, progressive decline in drug therapy can be attempted. However, most patients need to resume medication within 1 year.
PATIENT EDUCATION GUIDELINES :
PATIENT EDUCATION GUIDELINES Following the DASH eating plan DASH Dietary Approaches to Stop Hypertension Based on 2,000 calories per day diet Depending on patient’s caloric needs, the number of daily servings may vary For more information, log on to http://www.nhlbi.nih.gov/health/public/heart/hbp/dash.
NURSING ASSESSMENT :
NURSING ASSESSMENT Nursing History Family history of high BP Previous episodes of high BP Dietary habits and salt intake Cigarette smoking Episodes of headache, weakness, muscle cramp, tingling, palpitations, sweating, vision disturbances Medication that could elevate BP Hormonal contraceptives, steroids NSAIDs, Nasal decongestants, appetite suppressants
NURSING ALERT :
NURSING ALERT The finding of an isolated elevated BP does not necessarily indicate hypertension. However, the patient should be regarded as at risk for high BP until further assessment through history taking, repeat BP measurements, and diagnostic testing either confirms or denies the diagnosis
NURSING DIAGNOSES :
NURSING DIAGNOSES Deficient Knowledge regarding the relationship between the treatment regimen and control of the disease process Ineffective Therapeutic Regimen Management related to medication adverse effects and difficult lifestyle adjustments
NURSING INTERVENTIONSProvide basic education :
NURSING INTERVENTIONSProvide basic education Explain the meaning of high BP, risk factors Stress that there can never be total cure, only control can be done Stress the fact that there may be no correlation between high BP and symptoms Have the patient recognize that hypertension is chronic and requires persistent therapy and periodic evaluation.Effective treatment improves life expectancy
CONTD… :
CONTD… Explain the pharmacologic control of hypertension:- Explain that the drugs used for effective control of elevated BP will likely produce adverse effects. Warn the patient of the possibility that orthostatic hypotension may occur initially with some drug therapy Instruct the patient to get up slowly to offset the feeling of dizziness Encourage the patient to sit or lie down immediately if he feels faint Alert the patient to expect initial effects, such as anorexia, light-headedness, and fatigue, with many medications
GERONTOLOGIC ALERT :
GERONTOLOGIC ALERT Polypharmacy, cognitive changes, and sensory deficits in the elderly may make dosage adjustment and control of BP difficult. Work with the patient, family, and home care nurse to devise a simple method for the patient to take the proper medications. Elderly patients are also more sensitive to therapeutic levels of drugs and may demonstrate adverse effects while on an otherwise average dosage.They may be more sensitive to postural hypotension and should be cautioned to change positions with great care.
ACCELERATED HYPERTENSION :
ACCELERATED HYPERTENSION
DEFINITION :
DEFINITION Also called as Malignant Hypertension Occurs when B.P. elevates extremely rapidly Threatens one or more target organs like brain, heart & kidney.
PATHOPHYSIOLOGY :
PATHOPHYSIOLOGY
CLINICAL MANIFESTATIONS :
CLINICAL MANIFESTATIONS Brain effects: Encephalopathy Stroke Progressive headache, stupor, seizures Kidney effects: Decreased blood flow, vasoconstriction BUN elevated Plasma renin activity increased Urine specific gravity lowered Proteinuria Renal failure Cardiac effects: Left-sided heart failure Acute MI Right-sided heart failure
MANAGEMENT :
MANAGEMENT Immediate hospitalization and treatment if the following are present Seizures Abnormal neurologic signs Severe occipital headache Pulmonary edema The patient is hemodynamically monitored in the ICU Antihypertensive agents are administered parenterally. Agents include: Vasodilators Adrenergic inhibitors short-acting calcium antagonist Diuretics
NURSING ALERT :
NURSING ALERT BP should be reduced gradually and wide pressure variations avoided because lowered BP may not be adequate to perfuse vital organs
NURSING INTERVENTIONS :
NURSING INTERVENTIONS Record BP frequently Monitor for adverse effects of medications: headache, tachycardia, orthostatic hypotension Measure urine output accurately Observe for hypokalemia, especially if patient is placed on diuretic therapy. Monitor for ventricular dysrhythmias
THANKS :
THANKS

Gingivitis aggravated by systemic disease
Endocrine Disturbance and Hormonal Changes: Endocrine Disturbance and Hormonal Changes Diabetes Mellitus Complex metabolic disorder: diminished insulin production, impaired insulin action or combination of both result inability of glucose to be transported from blood to tissue resulting in high blood glucose level & secretion of glucose in urine
Lipids and proteins metabolism are disturbed as well Type I: insulin dependant: cell mediated autoimmune destruction of beta cells of islets of langerhans in pancreas. Children & young adults, difficult to control, unstable, ketosis & coma
Type II (NIDDM): peripheral resistance to insulin action, impaired secretion & increased glucose production, adult onset, obese individuals, can be controlled by diet & oral hypoglycemic agents
Long term complications of Diabetes: Long term complications of Diabetes Microvasculature Macro vasculature Increased liability to infection Poor wound healing
Oral manifestations: Oral manifestations Chelosis Dry mucosa Burning mouth and tongue Diminished salivary flow Altered oral flora: Candida albicans, hemolytic streptococcus Increased caries
Gingival inflammation, bleeding, and mobile teeth: A&B : Gingival inflammation, bleeding, and mobile teeth: A&B Tendency toward enlarged gingiva: fig C & D Abscess formation: fig E
Periodontitis in type I: Periodontitis in type I Start after age of 12 (9%) Prevalence increased with age (39%) at age of 19 Sever inflammation, deep pockets, rabid bone loss & frequent periodontal abscess
Higher Incidence of Periodontal Disease in Diabetes: Higher Incidence of Periodontal Disease in Diabetes Well controlled studies showed higher incidence of periodontal diseases in diabetic patients. 1- Bacterial pathogens: increased glucose in blood & gingival fluid change the environment of microbiota ( Capnocytophaga , anaerobic vibrios , actinomyces species)
2-Polymorphonuclear leukocyte function: 2-Polymorphonuclear leukocyte function Increased susceptibility of diabetic patients to infection may be related to: Decreased number of neutrophyles impaired chemotaxis defective phagocytosis, or impaired adherence
3-Altered Collagen Metabolism: 3-Altered Collagen Metabolism Chronic hyperglycemia adversely affects the synthesis, maturation and maintenance of collagen and extracellular substance 1- Decreased collagen activity 2-Increased collagenase activity 3-Excessive accumulated glycation end products (AGEs)
AGE cross linked collagen leading to less soluble, which is less liable to repair and leads to impaired cellular migration, impaired tissue integrity and less resistance to infection
Hormonal Imbalance: Hormonal Imbalance Female sex hormone: 1- The gingiva in puppetry : Puppetry is associated with an exaggerated response of the gingiva to plaque Pronounced inflammation, bluish red discoloration, edema and gingival enlargement
Gingiva in puppetry: Gingiva in puppetry
2-Gingival changes associated with Menstrual cycle: 2-Gingival changes associated with Menstrual cycle Prevalence of gingivitis increased in some patients with bleeding & tense feeling in the gum
3- Gingival Changes during pregnancy: 3- Gingival Changes during pregnancy Pregnancy affects the severity of previously inflamed areas; it does not alter healthy gingiva The severity increased during second or third month and become more severe by the 8 th month Partial reduction of severity occurs by 2 month postpartum
Clinical features of pregnancy gingivitis: Clinical features of pregnancy gingivitis Bright red to bluish color (vascularity) Edema that pits on pressure Smooth & shiny Bleeding tendency Enlargement All these changes can be generalized or localized
Etiologic significance: Etiologic significance Possibility of bacterial hormonal interaction that may change bacterial composition P intermedia was found to be associated with elevated levels of estradiol & progesterone It has also been reported that a depression of maternal T-lymphocyte response
The aggravated response in pregnancy has been attributed principally to increased level of progesterone, which produce dilatation of gingival microvasculature, circulatory stasis and increased susceptibility to mechanical irritation
4-Hormonal contraceptives & the gingiva: 4-Hormonal contraceptives & the gingiva Increased periodontal destruction after about one & half year of taking contraceptives was reported
5-Menoposal Gingivostomatitis: 5-Menoposal Gingivostomatitis Also termed “ senile atrophic stomatitis ” During menopause hormonal fluctuations of female cycle are ended as estradiol ceases to be major circulating estrogen Gingiva & oral mucosa are dry and vary in color from pale to red, fissuring of mucobuccal folds, ulcerations may be seen
Some of the signs and symptoms of diabetes:

Fatigue and tiredness

Thirsty and dry mouth

Blurry vision
Wounds that won’t heal

Always hungry

Numb or tingling hands/feet

Vaginal infections

Frequent urination


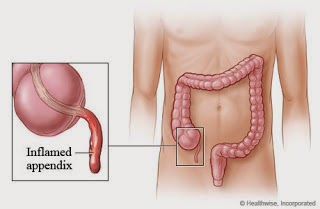

In February 2017, my immune system was not functioning correctly and my primary care physician did a N.A.E.T. Treatment with Laser Acupuncture and Auricular Acupuncture to try to desensitize my body from the different allergies and allergies to the metals. This procedure began to make me drained and very fatigued. He recommended that I have a GI Stool test done as I was having GI issues in February 2017, to check for parasites, pathogens, bacterial flora, and fungi/yeasts. The results showed that I had a Bacterial Pathogen called Salmonella, high amounts of normal bacterial flora, called Enterococcus spp. and Escherichia spp., 2 parasites called Dientamoeba fragilis and Endolimax nana, and 2 types of fungi/yeasts called Candida spp. and Geotrichum spp. The doctor recommended that I take Dr Itua Herbal Medicine to get rid of the Candida as that was the main concern at the time and I did purchase Dr Itua Herbal Medicine and after taking it all as instructed I was totally cured so is a urged form of heart to believe in herbal medicines but yes indeed natural remedies should be recognize around the globe because is the only healing that has no side effect on each every healing, I will recommend anyone here with health challenge to contact Dr Itua Herbal Center on E-Mail drituaherbalcenter@gmail.com / Www.drituaherbalcenter.com he capable of all kind of disease like Cancer,Hiv,Herpes,Kidney disease,Parkinson,ALS,Copd. with a complete cure without coming back.
ReplyDelete